
Statin Therapy for Patients with Cardiovascular Disease
Clinical Basis
Cardiovascular disease is the leading cause death in the United States. It is estimated that 126.9 million American adults have one or more types of cardiovascular disease.1
Exclusions
- Cirrhosis (K74.6)
- ESRD (N18.6) or Dialysis (dependence on renal dialysis, Z99.2)
- Hospice, palliative care
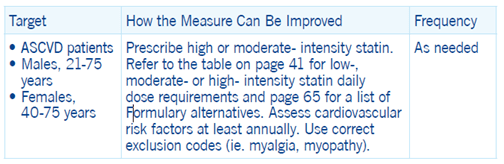
- Myalgia (M79.1), myositis (M60.9), myopathy (G72.9) or rhabdomyolysis (M62.82)
- Pregnancy, clomiphene use, or in vitro fertilization
- 66 years of age and older in I-SNP or living long-term in an institution
- 66 years of age and older with frailty and advanced illness
Other exclusions may apply
Important guidelines for your practice
The ACC/AHA guideline emphasizes that lifestyle modification remains a critical component of ASCVD reduction.2
Statin therapy is recommended in the following four groups:3
- Patients with any form of clinical ASCVD
- Patients with primary LDL-C levels of 190mg per dL or greater
- Patients with diabetes mellitus, 40 to 75 years of age, with LDL-C levels of 70 to 189mg per dL
- Patients without diabetes, 40 to 75 years of age, with an estimated 10-year ASCVD risk of at least 7.5 percent
The guideline recommends reducing ASCVD risk with high-intensity or maximally tolerated statin intensity with the goal of achieving 50% or greater reduction in LDL-C levels from baseline.
Risk assessment for 10-year and lifetime risk is recommended using an updated ASCVD risk calculator (https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/).
Recommendations resulted from expert panel reviews of multiple meta-analysis and RCTs including:
- In adults with coronary heart disease, statin therapy reduced the relative risk for cardiovascular events by 21 percent per 38.7mg/dL LDL-C reduction.
- In adults with and without cardiovascular disease who received more intensive statin therapy the risk for cardiovascular disease mortality was further reduced by 15 percent per 38.7mg/dL LDL-C reduction compared to standard statin therapy.4
High-intensity statins are recommended for patients with clinical ASCVD. As some patients may experience statin associated side effects; SPC permits moderate-intensity statins.
1 Tsao CM et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8): e153-e639.
2 Grundy SM et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA /ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082– e1143.
3 See section 4, Statin Treatment Recommendations in the 2018 ACC/AHA Cholesterol Guideline on Secondary Prevention in Patients with ASCVD for discussion of individual treatment options.
4 Cholesterol Treatment Trialists’ Collaboration, Baigent C, Blackwell L. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomized trials. Lancet 2010;376:1670–81