Kidney Disease Monitoring
Clinical Basis
Diabetic kidney disease, or kidney disease attributed to diabetes, occurs in 20 percent to 40 percent of patients with diabetes. Diabetic kidney disease is the leading cause of end-stage renal disease (ESRD).

Clinical Guidelines
- Optimize glucose control to reduce the risk or slow the progression of diabetic kidney disease [A].
- Optimize blood pressure control (< 140/90mmHg) to reduce the risk or slow the progression of diabetic kidney disease [A].
- For patients with non-dialysis-dependent diabetic kidney disease, dietary protein intake should be 8g/kg body weight per day (this is the recommended daily allowance). For patients on dialysis, higher levels of dietary protein intake should be considered [A].
- For treatment of non-pregnant patients with diabetes and modestly elevated urinary albumin excretion (30-299mg/day), either an angiotensin converting enzyme (ACE) inhibitor or an angiotensin receptor blocker is recommended [B].
- For treatment of patients with urinary albumin excretion³ 300mg/day and/or estimated glomerular filtration rate < 60 mL/min/1.73m2, either an ACE inhibitor or an angiotensin receptor blocker is strongly recommended [A].
- Periodically monitor serum creatinine and potassium levels for the development of increased creatinine or changes in potassium when ACE inhibitors, angiotensin receptor blockers or diuretics are used.
- Monitor the urinary albumin-to-creatinine ratio in patients with albuminuria treated with an ACE inhibitor or an angiotensin receptor blocker to assess the response to treatment and progression of diabetic kidney disease.
- An ACE inhibitor or an angiotensin receptor blocker is not recommended for the primary prevention of diabetic kidney disease in patients with diabetes who have normal blood pressure, normal urinary albumin-to-creatinine ratio (< 30mg/g) and normal estimated glomerular filtration rate [B].
- Evaluate and manage potential complications of chronic kidney disease when the estimated glomerular filtration rate is < 60 mL/min/1.73m2.
- Refer patients for evaluation for renal replacement treatment if they have estimated glomerular filtration rate < 30 mL/min/1.73m2 [A].
- Promptly refer patients to a physician experienced in the care of kidney disease when there is [B]:
- Uncertainty about the etiology of kidney disease
- Difficulty with management issues
- Rapidly progressing kidney disease
Screening Recommendations
Screen members once a year as follows [B]:
- All patients with type 2 diabetes
- All patients with comorbid hypertension
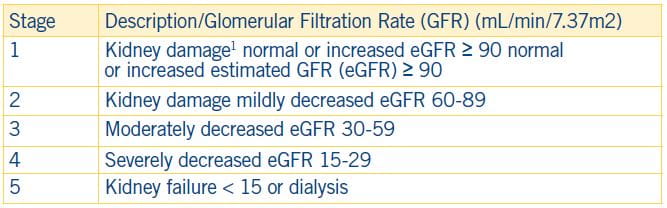
Stages of Chronic Kidney Disease